Metastatic Small Cell Carcinoma as a "Butterfly" Tumor of the Corpus CallosumKeywords: lung cancer, brain metastasis, glioblastoma multiforme, brain tumor, stereotactic biopsyInteractive ManuscriptAsk Questions of this Manuscript: What is the background behind this topic?It is commonly believed that the only tumors which can appear as bilateral ("butterfly") lesions of the corpus callosum are central nervous system lymphomas or malignant gliomas. Describe your observation(s).We performed a stereotactic biopsy in an 80 year-old woman who presented with an expanding symmetrical mass in the splenium of the corpus callosum who presented with short-term memory loss. During her evaluation, a hilar chest mass was found. Biopsy was performed because the imaging was inconsistent with her pulmonary lesion. The stereotactic brain biopsy showed metastatic small cell carcinoma, likely of lung origin. All glial markers and T-cell or B-cell markers were negative. Describe the major lesson provided by your observation.The differential diagnosis of bihemispheric callosal mass lesions should include metatstatic small cell carcinoma.This finding supports consideration of a metastatic work-up for patients with similar lesions. What is the background of your topic ?The finding on imaging of a bi-hemispheric callosal mass lesion, either in the genu, body, or splenium heralds the diagnosis of either a glioma or CNS lymphoma. Histologic confirmation is performed to distinguish between these entities or to grade a glial tumor. Other histologies are considered "almost impossible" to result in this imaging finding, and this "dogma" is a part of training. Describe your main observation and why it is important.We performed a stereotactic biopsy in an 80 year-old woman who presented with an expanding symmetrical mass in the splenium of the corpus callosum who presented with short-term memory loss. During her evaluation, a hilar chest mass was found. She was kept off corticosteroids to reduce the chance that a lymphoma might be hard to define with imaging. Her first magnetic resonance imaging scan (MRI) was performed without contrast. She was admitted for an MRI-guided stereotactic biopsy, with contrast that showed the callosal lesion as well as a small 1 cm ring enhancing lesion in the anterior right frontal lobe. The frontal lobe lesion remained consistent with a CNS lymphoma or a multicentric glioma, in addition to other pathologies.
The stereotactic brain biopsy of the right splenial mass showed metastatic small cell carcinoma, likely of lung origin. All glial markers and T-cell or B-cell markers were negative. Has this observation been reported previously?This observation has not been previously reported. If your work has Institutional Review Board or other supervisory authority approval, state that now:This work was approved by the University of Pittsburgh Institutional Review Board. State the source of funding for this study.This study was not funded by any external source. Describe how your observation was made (ie. specific tests, other)The observations in this study were made with two MRI scans and with tissue obtained via stereotactic biopsy. Describe the most important lesson(s) of this report.The corpus callosum is composed of dense myelinated fibers that connect regions of the two cerebral hemispheres. It is believed that this density serves as a blockage to tumor spread or flow of edema and, thus, only high-grade, aggressive tumors such as lymphoma of glioblastoma multiforme, cross the corpus callosum and cause the typical "butterfly" appearance. 1,2. The importance of this finding is that clinicians should be aware of the possibility for metastatic small cell carcinoma to mimic the appearance of a CNS lymphoma or glioblastoma of the corpus callosum. Describe the limitations of your findings.This finding still remains a rare possibility in the differential diagnosis of bihemispheric callosal tumors. Discuss the relevance of your observation to the reader.Not all lesions of the corpus callosum are necessarily GBM or lymphoma. Demylinating diseases can manifest in this region and appear as a pseudo-butterfly glioma. 3,4. Rare diseases, such as granuloctyic sarcoma or myeloid sarcoma taking the form of an enhancing "butterfly" lesion of the corpus have been reported.5,6. Infection, in particular, toxoplasmosis mimicking lymphoma in an HIV patient, can appear as a butterfly lesion. 7. We present a case of biopsy-proven metastatic non-small cell lung cancer presenting in the same manner. Therefore, as part of the evaluation of a bihemispheric callosal tumor, the patient should undergo a typical metastatic work-up, which includes imaging (x-ray or CT of the chest, CT of the abdomen and pelvis) to ensure that a primary cancer is not present. Typically a metastatic work-up is not performed in such patients. It is commonly believed that the only tumors which can appear as bilateral ("butterfly") lesions of the corpus callosum are central nervous system lymphomas or malignant gliomas. We performed a stereotactic biopsy in an 80 year-old woman who presented with an expanding symmetrical mass in the splenium of the corpus callosum who presented with short-term memory loss. During her evaluation, a hilar chest mass was found. Biopsy was performed because the imaging was inconsistent with her pulmonary lesion. The stereotactic brain biopsy showed metastatic small cell carcinoma, likely of lung origin. All glial markers and T-cell or B-cell markers were negative. The differential diagnosis of bihemispheric callosal mass lesions should include metatstatic small cell carcinoma.This finding supports consideration of a metastatic work-up for patients with similar lesions.
The finding on imaging of a bi-hemispheric callosal mass lesion, either in the genu, body, or splenium heralds the diagnosis of either a glioma or CNS lymphoma. Histologic confirmation is performed to distinguish between these entities or to grade a glial tumor. Other histologies are considered "almost impossible" to result in this imaging finding, and this "dogma" is a part of training. We performed a stereotactic biopsy in an 80 year-old woman who presented with an expanding symmetrical mass in the splenium of the corpus callosum who presented with short-term memory loss. During her evaluation, a hilar chest mass was found. She was kept off corticosteroids to reduce the chance that a lymphoma might be hard to define with imaging. Her first magnetic resonance imaging scan (MRI) was performed without contrast. She was admitted for an MRI-guided stereotactic biopsy, with contrast that showed the callosal lesion as well as a small 1 cm ring enhancing lesion in the anterior right frontal lobe. The frontal lobe lesion remained consistent with a CNS lymphoma or a multicentric glioma, in addition to other pathologies.
The stereotactic brain biopsy of the right splenial mass showed metastatic small cell carcinoma, likely of lung origin. All glial markers and T-cell or B-cell markers were negative. This observation has not been previously reported. Figure 1:
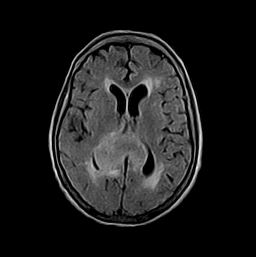 |
| Axial MRI (flair) showing a "butterfly" mass in the splenium of the corpus callosum. |
Figure 2: 2a
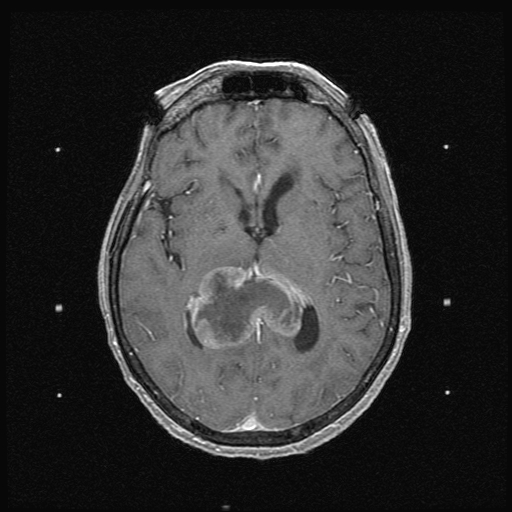 |
| Mass in the splenium of the corpus callosum. |
Figure 3: 2b
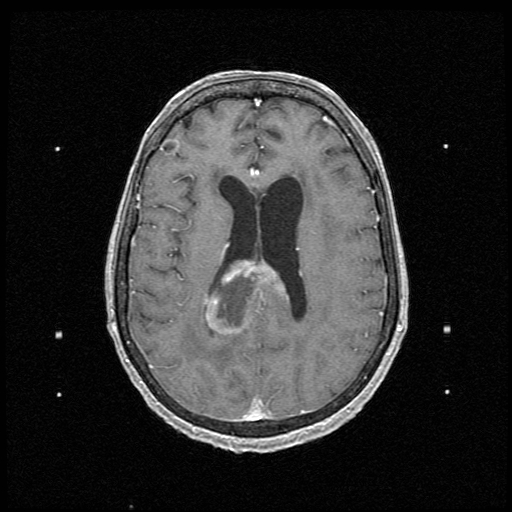 |
| Axial MRI showing a second tumor in the lateral right frontal lobe. |
Figure 4: 3
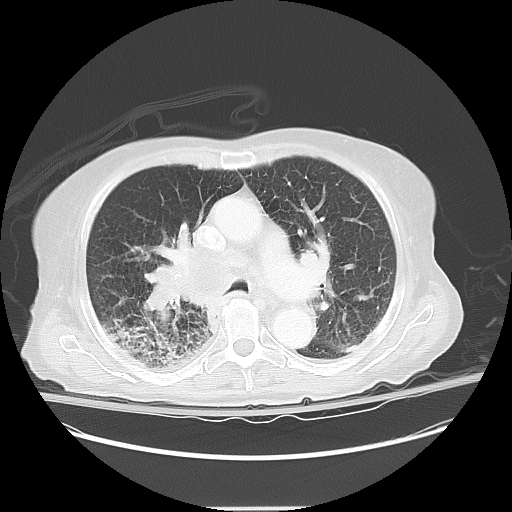 |
| CT of the chest showing the pulmonary mass. |
This work was approved by the University of Pittsburgh Institutional Review Board. This study was not funded by any external source. The observations in this study were made with two MRI scans and with tissue obtained via stereotactic biopsy. Figure 5: 4a
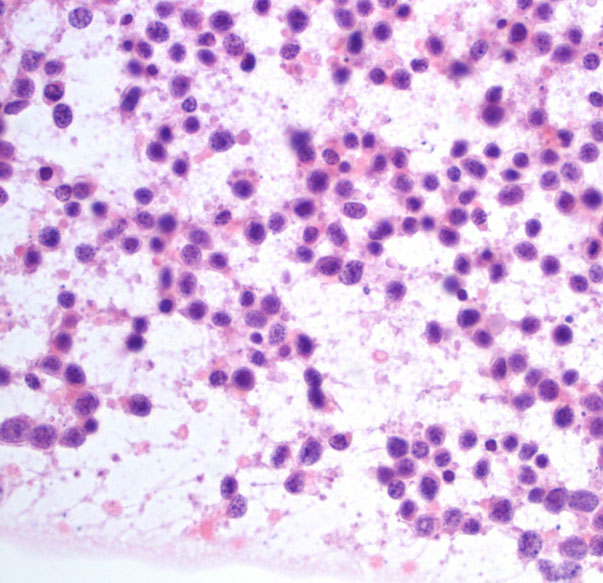 |
| smear: H&E stained smear shows discohesive pleomorphic round cells with variable chromatin pattern. This pattern is characteristic for lymphoma but can be seen sometimes in GBM and even metastatic carcinomas especially if partially necrotic |
Figure 6: 4b
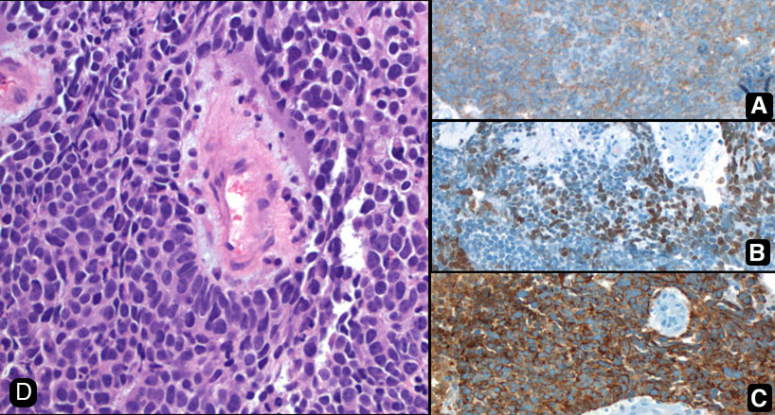 |
| paramontage: Paraffin permanent sections with immunostains. A. Synaptophysin (neruoendocrine marker), B. TTF-1 (neck and lung derivation marker), pankeratin (epithelial marker) D. H&E 40x |
The corpus callosum is composed of dense myelinated fibers that connect regions of the two cerebral hemispheres. It is believed that this density serves as a blockage to tumor spread or flow of edema and, thus, only high-grade, aggressive tumors such as lymphoma of glioblastoma multiforme, cross the corpus callosum and cause the typical "butterfly" appearance. 1,2. The importance of this finding is that clinicians should be aware of the possibility for metastatic small cell carcinoma to mimic the appearance of a CNS lymphoma or glioblastoma of the corpus callosum. This finding still remains a rare possibility in the differential diagnosis of bihemispheric callosal tumors. Not all lesions of the corpus callosum are necessarily GBM or lymphoma. Demylinating diseases can manifest in this region and appear as a pseudo-butterfly glioma. 3,4. Rare diseases, such as granuloctyic sarcoma or myeloid sarcoma taking the form of an enhancing "butterfly" lesion of the corpus have been reported.5,6. Infection, in particular, toxoplasmosis mimicking lymphoma in an HIV patient, can appear as a butterfly lesion. 7. We present a case of biopsy-proven metastatic non-small cell lung cancer presenting in the same manner. Therefore, as part of the evaluation of a bihemispheric callosal tumor, the patient should undergo a typical metastatic work-up, which includes imaging (x-ray or CT of the chest, CT of the abdomen and pelvis) to ensure that a primary cancer is not present. Typically a metastatic work-up is not performed in such patients.
The Author(s) wish to thank:Project Roles:
1. Agrawal, A., et al: Butterfly glioma of the corpus callosum.. J Cancer Res Ther. 5: 43 - 45, 20092. Alvarez, M., et al: Intracerebral granulocytic sarcoma. J Neurosci Nurs 39: 297 - 304, 20073. Bourekas, E.,Varakis, K.,Bruns, D., Lesions of the corpus callosum: MR imaging and differential considerations in adults and children.. Am J Roentgenol. 179: 251 - 257, 20024. Chaudhari, W.,Yim, C.,Hathout, H.,Lai, A.,Donovan, S., et al: Atypical imaging appearance fo toxoplasmosis in an HIV patient as a butterfly lesion. J Magn Reson Imaging 30: 873 - 875, 20095. Kei, P.,Kok, T.,Linn, Y.,Padhy, A., et al: Butterfly lesion of the corpus callosum: An unusual case of extramedullary myeloid sarcoma (granulocytic sarcoma). Clin Nuc Med 36: 365 - 366, 20116. Kiernan, M.,Vonau, M.,Bullpit, P.,Tohver, E.,Milder , D., et al: Butterfuly lesion of the corpus callosum due to Schilder's disease.. J Clin Neurosci 8: 367 - 369, 20017. Scozzafava, J.,Johnson, E.,Blevins, G., et al: Neurological picture. Demylinating butterfly pseudo-glioma.. J Neurol Neurosurg Psychiatry 79: 12 - 13, 2008
|
